Hinrichsen, C. Organ Histology. London: World Scientific Publishing Co, 1997.
Bittar, E.E.. Pulmonary Biology in Health and Disease. New York: Springer-Verlag New York, Inc., 2002.
Bailey, T.C. and Ruud A.W. Veldhuizen, “The Physiological Significance of a Dysfunctional Lung Surfactant”. Nag, Kaushik. Lung Surfactant Function and Disorder. Boca Raton, FL: Taylor & Francis Group, 2005. pp 359-381.
Negus, Sir V. The Biology of Respiration. Edinburgh: E. & S. Livingstone Ltd., 1965.
Pulmonary Alveolar Proteinosis (PAP) - Causes, Symptoms, Diagnosis, Treatment, Cures and Remedies for Pulmonary Alveolar Proteinosis. Retrieved on October 28th, 2009 from:
So there you have it, the respiratory alveoli! The functional unit of the lung explained in detail, for your understanding. I hope that you found this blog helpful and interesting, and that you gained an appreciation for how the respiratory system helps to provide a foundation for the workings of the body as a whole. Best wishes, and breath deep! =)
There exist a number of various pathologies associated with the alveolar structure, however, in this blog, only two will be discussed in detail. These include emphysema and pulmonary alveolar proteinosis, or PAP for short.
The first condition, emphysema, is characterized by the enlargement of the respiratory airspaces as a result of many destructive changes within the alveoli of the lungs. The basis for the classification of emphysema in an individual involves the localizations of lesions present onthe acinus, which consists of 3 to 5 orders of respiratory bronchioles, alveolar ducts, and alveoli (2). There is a large loss of the elastic recoil in the lungs, due to the disruption of elastic fibers, and as a result of these changes, the compliance as well as the diffusing capacity of the lungs are greatly decreased (2). One major cause of emphysema includes exposure to cigarette smoke throughout life (2).
Figure 7: Normal Alveoli vs. Alveoli with Emphysema
(Retrieved from http://media-2.web.britannica.com/eb-media/04/100104-036-0E044846.jpg )
The second condition, called PAP, is caused by an oversecretion of surfactant within the alveoli of the lung, which subsequently causes a reduction in the oxygen that is able to diffuse across the alveoli and on into the pulmonary capillaries for transport to the body (5). It occurs in men more so than women, and symptoms generally include a dry cough, weight loss, and a shortness of breath (5). The exact cause of PAP is unknown in many cases, however, there does appear to be genetic link, which can be hereditary (5).
Figure 8: Lung Showing the Presence of Increased Amounts of Surfactant
(Retrieved from http://www.ajronline.org/content/vol176/issue5/images/small/05_AA1162_05A.gif)
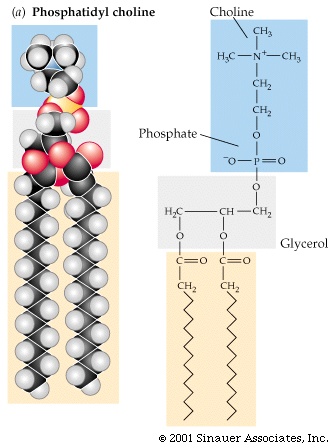
For the proper functioning of the respiratory alveoli, a number of different required compounds must be secreted from the cells that comprise the structure of the alveoli. One such essential fluid is known as surfactant, and it is secreted primarily by the Type-II cells (2). This fluid is made from a variety of compounds of which 85% are phospholipids, 10 % are surface-associated proteins, and 5% are neutral lipids such as cholesterol (3). Where the phospholipids are concerned, the main contribution to this group is made by phosphatidylcholine as it accounts for roughly 60% of the phospholipids found in the surfactant (3).
The role of surfactant in the lung is considered two-fold. First, surfactant is a structural aid in that it increases lung compliance, reducing the amount of pressure required to inflate the lungs during inhalation, while also reducing the surface tension at the air-liquid interface (3). This reduction in the surface tension of the alveoli prevents their collapse, which is known as atelectasis (1). The second function of surfactant is to help with innate immune defense, protecting against possible invaders within the respiratory system (3).
Figure 6: The Molecule Phosphatidylcholine Found in Surfactant (Retrieved from http://www.columbia.edu/cu/biology/courses/c2005/purves6/figure03-21.jpg)
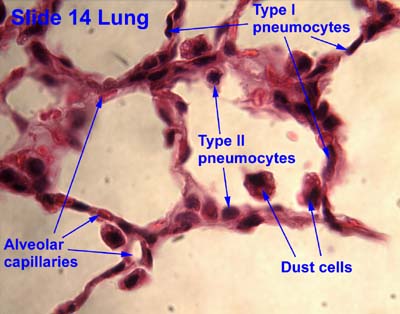
Within the alveoli exist several different types of cells which all aid in the proper functioning of the respiratory alveoli in gas exchange. These cell types include:
• Type-I Cells: also called Type I pneumocytes or pulmonary epithelial cells (1), these cells are squamous and comprise approximately 40% of the cells present in the alveolar lining (2). They contain a centrally located flat nucleus which is closely surrounded by the few organelles that it does contain (2). Each of these cells has a diameter of roughly 50µm, and as such these cells cover over 90% of the alveolar surface (2). The main role of these cells is to provide a very surface that is easily permeated for the simple diffusion of gases as they are the cells that are in the greatest contact with air (4).
• Type-II Cells: These cells may also be referred to as great alveolar cells or Type II pneumocytes (1). These cells are generally round or cuboidal in shape with a diameter of no more than 15µm, and comprise 60% of the alveolar cells, but only account for about 5% of the surface area (2). They contain a large basal nucleus, which has a very prominent nucleolus, large amounts of cytoplasm, and well developed organelles like the endoplasmic reticulum and Golgi apparatus (2) that are involved in secretion (1). These cells also contain lamellar inclusion bodies which contain phospholipids, mucopolysaccharides, proteins and lysosomal hydrolases, and are producers of surfactant (1). Another important feature of these cells is that they aid in repairing and remodeling the lung, and act as reserve cells to replenish lost Type-I cells (2).
• Alveolar Macrophages: Also known as dust cells, these cells originate from the monocytic series of the bone marrow, and are large, free moving phagocytes present on the alveolar surfaces (1 & 2).They contain processes called pseudopods, and contain lysosomes used to break down phagocytosed invaders and damaged or dead tissue (2). As this suggests, the primary function of these cells is to defend the respiratory system against infection or contamination by foreign compounds and/or organisms that we inadvertently inhaled (1). They also contain inflammatory mediators, and have very well developed organelles (2).
Also, it may be noted that both Type I and II cells are joined by tight junctions, and are attached to a very well developed basal lamina, thus preventing the leakage of any molecules which have a molecular weight higher than 1000 kDa.
Figure 4: Types of Cells in Alveoli (Retrieved from
In mature adults, the alveoli are found in bunches of anywhere from 2 to 5 alveoli, situated at the terminal ends of the terminal bronchioles in polyhedral sacs called atria (1). Generally each individual alveolus is in the vicinity of 300 µm in diameter (1), and with approximately 300 million alveoli found in the lungs of a 70 kg man, they provide a total surface area of roughly 143 square meters for gas exchange (2). This gas exchange of carbon dioxide and oxygen within the alveoli during respiration, occurs across what is referred to as the air-blood barrier. The pulmonary capillary network is the most extensive network of capillaries within the body, and covers rough 85-95% of the surface of the alveoli (2). In fact, it has a surface area of 126 square meters! Which is 70 times the surface area of skin! (2)
The interalveolar walls of the alveoli are made from an epithelium which is covering a highly vascularized space of connective tissue (1). This connective tissue space includes the following types of structures (1):
Also, as a result of their development, alveoli also have pores which connect them to other alveoli which are adjacent. These pores are generally 7-9µm in diameter and allow for the collateral circulation of air, which aids to prevent the collapse of the alveoli in the event of a proximal blockage (1). It may also be noted, that these pores arise in conjunction with maturity, and are not found in the fetal lung (2).
The alveoli begin development approximately 4 to 6 months into pre-natal development, when the respiratory bronchioles form through the branching of both bronchi and the bronchioles (1). This stage, called the canalicular stage, sees the formation of what is to become the air-blood barrier, as well as the differentiation of the columnar pulmonary epithelial cells into Type II and Type I cells (1). The synthesis of surfactant also begins late in this stage of development, and during a brief period both before and after birth (approximately 1 month), a sharp increase in the number of alveolar macrophages is also exhibited (1).
Over the course of the period from 6 months to birth, the alveolar ducts begin branching, and continue to do so for about 8 years after the birth of the child (1). The primary septa, which are located between air spaces within the lung, are comprised of a layer of connective tissue which has on both sides, a layer of capillaries. In the several days following birth, one of these capillary beds gives rise to a secondary septa through the process of upfolding, and it will be these septa that, with the formation of elastic tissue, give rise to the alveoli of the lung (1).
Figure 2: Composition of the Alveoli (Retrieved from
Within the human body, there exist a large variety of different tissues organized into organs and organ systems, which provide the means necessary to support life as we know it. Through interactions involving such important systems, acquisition of the substances required for life, and determination of how these substances are to be used, can be achieved.
However, it seems that there are some systems which are fundamental to life, and represent the foundation around which many of the other systems are built. One of these systems in particular is the respiratory system; the means by which gas exchange occurs in the body. This system is dynamic in every sense, containing a multitude of cell types which all have specific, yet complimentary, roles to carry out. While complex, the respiratory system carries out gas exchange by means of its functional unit, the respiratory alveoli, the primary focus of this blog. Here, the developmental, structural, cellular, functional, and pathological characteristics of the alveoli will be discussed with the aim that you will gain a better understanding of how this tiny integral part of life works.






{kind=link}