Acta Anaesthesiologica Scandinavica 2009; 1-8
Introduction
In this paper, Wu et al. (2009) examine the effect of surfactant replacement on the overdistension of terminal airspaces, and plasma cytokine levels in the lungs, caused by ventilator-induced lung injury, also known as VILI. This particular disorder is characterized by the overdistension of the lungs as a result of high pressure ventilation, or HPV, by usage of large tidal (inspiration/expiration) volumes during ventilation, and repetitious opening and closing of atelectatic lungs units, putting these units under considerable stress. From a pathological standpoint VILI shares many similarities with acute respiratory distress syndrome (ARDS). In this respect, symptoms include abnormalities in lung surfactant (that can decrease lung function) and increased activity (upregulation) of cytokines responsible for inflammation processes. The latter can also cause injury in organs other than the lungs. These symptoms are a direct cause of lung overdistension, that alters the cytoskeletal structure of the lung tissue, causes stress failure in cell membranes, and initiates the signaling cascades and gene expression pathways of inflammation processes.
Method
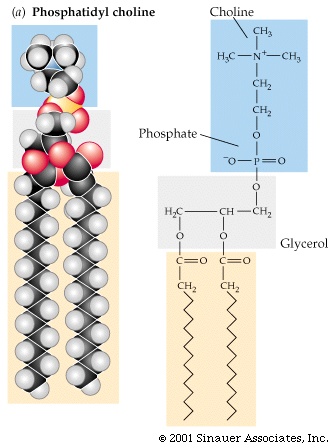
To begin, Wu et al. (2009) isolated a modified natural surfactant from alveolar lavage fluid of pigs. This Modified natural surfactant (MNS) contained, by weight, 98.0% phospholipids, 0.9% other lipids, and 1.1% surfactant proteins B and C. They noted that in a previous study, this MNS was shown to have a capacity similar to Curosurf for beneficial effects on surfactant deficient animals.
In this study, Wu et al. (2009) utilized 28 Wistar rats, ranging in weight from 310 to 388 grams. For the experiment, each rat was anesthetized using pentobarbital sodium (50 mg/kg i.p.). In addition, 1-2 ml of 0.5% lidocaine was administered as a local anesthetic for the purpose of a skin incision. Rat body temperature was kept at 37.0-38.5°C, a tracheotomy was performed, and the femoral artery was cannulated for blood pressure and samples.
Before ventilation procedures, 7 rats were killed at random (by exsanguination) to act as a control group for the experiment. The remaining 21 rats were subjected to ventilation procedures, which initially consisted of a ventilator providing a 10 ml/kg tidal volume (no positive end-expiratory pressure), at 45 breaths per minute, with 1 expiration to 1 inspiration, and 100% oxygen. Saline and a muscle relaxant were given, and partial pressures of oxygen and carbon dioxide were determined. Finally, the base lung-thorax compliance value was found by manually injecting 4 ml/kg of air into the lungs.
Next, the 21 rats were subjected to high pressure ventilation at 20 breaths per minute with 100% oxygen. The peak inspiration pressure was set at 40 cmH2O, while positive end-expiratory pressure was maintained at 0 cmH2O, with lung thorax compliance checked regularly. After once again placing the rats on the volume-controlled ventilator, Wu et al. (2009) increased the positive end-expiratory pressure in a stepwise manner, after which the rats were randomly placed in groups of seven as follows:
- Non-ventilated: Killed at the outset to act as control group for all aspects of the experiment.
- HPV-only: Killed immediately after subjection to ventilation procedure. Used to determine effect of surfactant, and levels of cytokines.
- Surfactant: Subjected to ventilation procedure in the same fashion as the placebo group. However, these rats were given 2 ml/kg of MNS suspensions. Killed two hours after administration of the surfactant.
- Placebo: Subjected to ventilation procedure in the same fashion as the surfactant group. These rats were given 2 ml/kgof air as opposed to the MNS suspension. Killed 2 hours after exposure to air.
The rats were killed by exsanguination, and both blood and tracheal fluid samples were collected. Lung volumes were measured and transverse sections of the lungs were fixed and stained with H&E. Terminal airspaces were measured using the slides and a computer program. Tracheal fluid protein concentration was measured with commercially available means, while an enzyme-linked immunosorbent assay measured plasma levels of TNF-alpha, MIP-2, IL-6 and IL-10.
Results
After exposure to the HPV procedure, Wu et al. (2009) found the mean values of the partial pressure of oxygen (PaO2) decreased from a baseline of over 500 mmHg to only 120 mmHg. However, treatment with surfactant raised the PaO2 to 422 mmHg 15 minutes post HPV, and maintained this level for approximately 2 hours, while the placebo only attained a PaO2 of 171 mmHg, post HPV. Notably, their surfactant group also showed lower PaCO2 and PIP values, and a higher mean arterial pressure than the placebo group.
For lung volume, the surfactant showed no large difference from that of the control group, while both the placebo and HPV-only groups had significantly lower volumes. Tracheal fluid amounts differed little after HPV, but 2 hours following surfactant/placebo addition, the researchers found the amount of tracheal fluid from the surfactant group was much lower than the placebo group, as were leukocyte numbers.
The representative lung sections (as per Figure 1) showed 60-80% of the airspaces in the HPV-only and placebo groups were in a near collapsed state. Also, 13.4% of the total airspaces in the control group were from the largest class of airspaces (class d), which compared to 16.1% in the surfactant group. These percentages were much lower than the 32.0% and 44.6% of the HPV-only and placebo groups respectively.

Figure 1: Representative lung sections fixed at 10 cmH2O on deflation. Open bars indicate 300 μm. Rats non-ventilated (N) and exposed to high-pressure ventilation (HPV); H, HPV-only group; S, surfactant group; P, placebo group.
(Figure and caption retrieved from http://www3.interscience.wiley.com/cgi-bin/fulltext/122600820/main.html,ftx_abs)
Next, there was no difference in the TNF-alpha levels of the groups. However, MIP-2 plasma levels, while below detection limit in the control, were 6.9 ng/ml in the HPV-only group. The quantity of MIP-2 increased to 11.8 and 12.5 ng/ml in the surfactant and placebo groups respectively, with IL-6 and IL-10 levels exhibiting comparable patterns.
In summation, the study showed that HPV induces a decrease of dissolved gases in arterial blood, the creation of a protein rich tracheal fluid, enlarged and collapsed terminal airspaces, and reduced lung volume. Subsequent treatment with surfactant appeared successful in reversing these changes and preventing atelectasis. However, the surfactant addition did not alter plasma MIP-2, IL-6, and IL-10 levels.
As and aside, Wu et al. (2009) suggest that supplementary experimentation is evidently necessary to fully understand the implications of surfactant replacement therapy for the treatment of VILI. To begin, they understand that the model used in this experiment may not accurately depict a clinical situation. Also, that the MNS used for this study did not contain surfactant proteins A and D, which normally have immune action and can cause inhibition of mediator release from active inflammatory cells.
My Opinion
In providing a critique of this paper, it is evident that Wu et al. (2009) had laid out very clear guidelines as to the experimental approach that would be taken over the course of the investigation. Not only were their intentions clearly expressed, and their discussion easy to follow, the supporting figures were clearly labeled and easily interpreted provided the reader had some scientific knowledge (ie. biology or biochemistry). Their methodology was very clear, very detailed, and appeared to be robust, such that anyone else wishing to reproduce the experiment, could do so with the right equipment under any number of conditions.
The results that were obtained by Wu et al. (2009) appear very promising in the alleviation of symptoms associated with VILI, and have the potential to completely abolish this problem in the future. That being said though, I must commend the researchers for finding shortcomings in their own work. It would be very beneficial to explore the effects of a surfactant containing both surfactant proteins A and D to see whether they held any helpful or negative effects on treating VILI, in particular diminishing the effects of cytokines and other inflammatory particles.
An area which was of some concern in my opinion, were the experimental subjects used. While rats are readily available, use of specimens more closely related to human physiology may have better represented a clinical scenario. For example the use of pigs or primates would have been ideal. However, in such a case, modifications to the experiment would have to be made to ensure that procedures were conducted as humanely as possible.
Overall, Wu et al. (2009) gave excellent insight into how VILI could potentially be treated. This paper has opened many possibilities for research into this area, and the outlook seems very promising.







{kind=link}